Mendelian randomization suggests a bidirectional, causal relationship between physical inactivity and adiposity
Curation statements for this article:-
Curated by eLife

Evaluation Summary:
The manuscript by Carrasquilla and colleagues applied Mendelian Randomization (MR) techniques to study causal relationship of physical activity and obesity. Their results support the causal effects of physical activity on obesity, and bi-directional causal effects of sedentary time and obesity. One strength of this work is the use of CAUSE, a recently developed MR method that is robust to common violations of MR assumptions. The conclusion reached could potentially have a large impact on an important public health problem.
(This preprint has been reviewed by eLife. We include the public reviews from the reviewers here; the authors also receive private feedback with suggested changes to the manuscript. Reviewer #2 and Reviewer #3 agreed to share their name with the authors.)
This article has been Reviewed by the following groups
Discuss this preprint
Start a discussion What are Sciety discussions?Listed in
- Evaluated articles (eLife)
Abstract
Physical inactivity and increased sedentary time are associated with excess weight gain in observational studies. However, some longitudinal studies indicate reverse causality where weight gain leads to physical inactivity and increased sedentary time. As observational studies suffer from reverse causality, it is challenging to assess the true causal directions. Here, we assess the bidirectional causality between physical inactivity, sedentary time, and adiposity by bidirectional Mendelian randomization analysis. We used results from genome-wide association studies for accelerometer-based physical activity and sedentary time in 91,105 individuals and for body mass index (BMI) in 806,834 individuals. We implemented Mendelian randomization using CAUSE method that accounts for pleiotropy and sample overlap using full genome-wide data. We also applied inverse variance-weighted, MR-Egger, weighted median, and weighted mode methods using genome-wide significant variants only. We found evidence of bidirectional causality between sedentary time and BMI: longer sedentary time was causal for higher BMI [beta (95% CI) from CAUSE method: 0.11 (0.02, 0.2), p = 0.02], and higher BMI was causal for longer sedentary time (0.13 (0.08, 0.17), p = 6.3 x 10 -4 ). Our analyses suggest that higher moderate and vigorous physical activity are causal for lower BMI (moderate: –0.18 (-0.3,–0.05), p = 0.006; vigorous: –0.16 (-0.24,–0.08), p = 3.8 × 10 -4 ), but indicate that the association between higher BMI and lower levels of physical activity is due to horizontal pleiotropy. The bidirectional, causal relationship between sedentary time and BMI suggests that decreasing sedentary time is beneficial for weight management, but also that targeting adiposity may lead to additional health benefits by reducing sedentary time.
Article activity feed
-

-

Author Response
Reviewer #2 (Public Review):
The manuscript by Carrasquilla and colleagues applied Mendelian Randomization (MR) techniques to study causal relationship of physical activity and obesity. Their results support the causal effects of physical activity on obesity, and bi-directional causal effects of sedentary time and obesity. One strength of this work is the use of CAUSE, a recently developed MR method that is robust to common violations of MR assumptions. The conclusion reached could potentially have a large impact on an important public health problem.
Major comments:
(1) While the effect of physical activity on obesity is in line with earlier studies, the finding that BMI has a causal effect on sedendary time is somewhat unexpected. In particular, the authors found this effect only with CAUSE, but the evidence …
Author Response
Reviewer #2 (Public Review):
The manuscript by Carrasquilla and colleagues applied Mendelian Randomization (MR) techniques to study causal relationship of physical activity and obesity. Their results support the causal effects of physical activity on obesity, and bi-directional causal effects of sedentary time and obesity. One strength of this work is the use of CAUSE, a recently developed MR method that is robust to common violations of MR assumptions. The conclusion reached could potentially have a large impact on an important public health problem.
Major comments:
(1) While the effect of physical activity on obesity is in line with earlier studies, the finding that BMI has a causal effect on sedendary time is somewhat unexpected. In particular, the authors found this effect only with CAUSE, but the evidence from other MR methods do not reach statistical significance cutoff. The strength of CAUSE is more about the control of false positive, instead of high power. In general, the power of CAUSE is lower than the simple IVW method. This is also the case in this setting, of high power of exposure (BMI) but lower power of outcome (sedentary time) - see Fig. 2B of the CAUSE paper.
It does not necessarily mean that the results are wrong. It's possible for example, by better modeling pleiotropic effects, CAUSE better captures the causal effects and have higher power. Nevertheless, it would be helpful to better understand why CAUSE gives high statistical significance while others not. Two suggestions here:
(a) It is useful to visualize the MR analysis with scatter plot of the effect sizes of variants on the exposure (BMI) and outcome (sedentary time). In the plot, the variants can be colored by their contribution to the CAUSE statistics, see Fig. 4 of the CAUSE paper. This plot would help show, for example, whether there are outlier variants; or whether the results are largely driven by just a small number of variants.
We agree and have now added a scatter plot of the expected log pointwise posterior density (ELPD) contributions of each variant to BMI and sedentary time, and the contributions of the variants to selecting either the causal model or the shared model (Figure 2-figure supplement 1 panel A). We identified one clear outlier variant (red circle) that we thus decided to remove before re-running the CAUSE analysis (panel B). We found that the causal effect of BMI on sedentary time remained of similar magnitude before and after the removal of this outlier variant (beta=0.13, P=6x10-4 and beta=0.13, P=3x10-5, respectively) (Supplementary File 1 and 2).
We have added a paragraph in the Results section to describe these new findings:
Lines 204-210: “We checked for outlier variants by producing a scatter plot of expected log pointwise posterior density (ELPD) contributions of the variants to BMI and sedentary time (Supplementary File 1), identifying one clear outlier variant (rs6567160 in MC4R gene) (Figure 2, Appendix 1—figure 2). However, the causal effect of BMI on sedentary time remained consistent even after removing this outlier variant from the CAUSE analysis (Supplementary File 1 and 2).”
(b) CAUSE is susceptible to false positives when the value of q, a measure of the proportion of shared variants, is high. The authors stated that q is about 0.2, which is pretty small. However, it is unclear if this is q under the causal model or the sharing model. If q is small under the sharing model, the result would be quite convincing. This needs to be clarified.
We thank the reviewer for a very relevant question. We have now clarified in the manuscript that all of the reported q values (~0.2) were under the causal model (lines 202-203). We applied the strict parameters for the priors in CAUSE in all of our analyses, which leads to high shared model q values (q=0.7-0.9). To examine whether our bidirectional causal findings for BMI and sedentary time may represent false positive results, we performed a further analysis to identify and exclude outlier variants, as described in our response to Question 7. I.e. we produced a scatter plot of expected log pointwise posterior density (ELPD) contributions of each variant to BMI and sedentary time, and the contributions of the variants to selecting either the causal model or the shared model (Supplementary Figure 2 panel A, shown above). We identified one clear outlier variant (red circle) that we thus removed (panel B), but the magnitude of the causal estimates was not affected by the exclusion of the variant (Supplementary File 1 and 2).
(2) Given the concern above, it may be helpful to strengthen the results using additional strategy. Note that the biggest worry with BMI-sedentary time relation is that the two traits are both affected by an unobserved heritable factor. This hidden factor likely affects some behavior component, so most likely act through the brain. On the other hand, BMI may involve multiple tissue types, e.g. adipose. So the idea is: suppose we can partition BMI variants into different tissues, those acted via brain or via adipose, say; then we can test MR using only BMI variants in a certain tissue. If there is a causal effect of BMI on sedentary time, we expect to see similar results from MR with different tissues. If the two are affected by the hidden factor, then the MR analysis using BMI variants acted in adipose would not show significant results.
While I think this strategy is feasible conceptually, I realize that it may be difficult to implement. BMI heritability were found to be primarily enriched in brain regulatory elements [PMID:29632380], so even if there are other tissue components, their contribution may be small. One paper does report that BMI is enriched in CD19 cells [PMID: 28892062], though. A second challenge is to figure out the tissue of origin of GWAS variants. This probably require fine-mapping analysis to pinpoint causal variants, and overlap with tissue-specific enhancer maps, not a small task. So I'd strongly encourage the authors to pursue some analysis along this line, but it would be understandable if the results of this analysis are negative.
We thank the reviewer for a very interesting point to address. We cannot exclude the possibility of an unobserved heritable factor acting through the brain, and tissue-specific MR analyses would be one possible way to investigate this possibility. However, we agree with the reviewer that partitioning BMI variants into different tissues is not currently feasible as the causal tissues and cell types of the GWAS variants are not known. Nevertheless, we have now implemented a new analysis where we tried to stratify genetic variants into “brain-enriched” and “adipose tissue-enriched” groups, using a simple method based on the genetic variants’ effect sizes on BMI and body fat percentage.
Our rationale for stratifying variants by comparing their effect sizes on BMI and body fat percentage is the following:
BMI is calculated based on body weight and height (kg/m2) and it thus does not distinguish between body fat mass and body lean mass. Body fat percentage is calculated by dividing body fat mass by body weight (fat mass / weight * 100%) and it thus distinguishes body fat mass from body lean mass. Thus, higher BMI may reflect both increased fat mass and increased lean mass, whereas higher body fat percentage reflects that fat mass has increased more than lean mass.
In case a genetic variant influences BMI through the CNS control of energy balance, its effect on body fat mass and body lean mass would be expected to follow the usual correlation between the traits in the population, where higher fat mass is strongly correlated with higher lean mass. In such a scenario, the variant would show a larger standardized effect size on BMI than on body fat percentage. In case a genetic variant more specifically affects adipose tissue, the variant would be expected to have a more specific effect on fat mass and less effect on lean mass. In such scenario, the variant would show a larger standardized effect size on body fat percentage than on BMI.
We therefore stratified BMI variants into brain-specific and adipose tissue-specific variants by comparing their standardized effect sizes on BMI body body fat percentage. Of the 12,790 variants included in the BMI-sedentary time CAUSE analysis, 12,266 had stronger effects on BMI than on body fat percentage and were thus classified as “brain-specific”. The remaining 524 variants had stronger effects on body fat percentage than on BMI (“adipose tissue-specific”). To assess whether the stratification of the variants led to biologically meaningful groups, we performed DEPICT tissue-enrichment analyses. The analyses showed that the genes expressed near the “brain-specific” variants were enriched in the CNS (figure below, panel A), whereas the genes expressed near the “adipose tissue-specific” variants did not reach significant enrichment at any tissue, but the showed strongest evidence of being linked to adipocytes and adipose tissue (figure below, panel B).
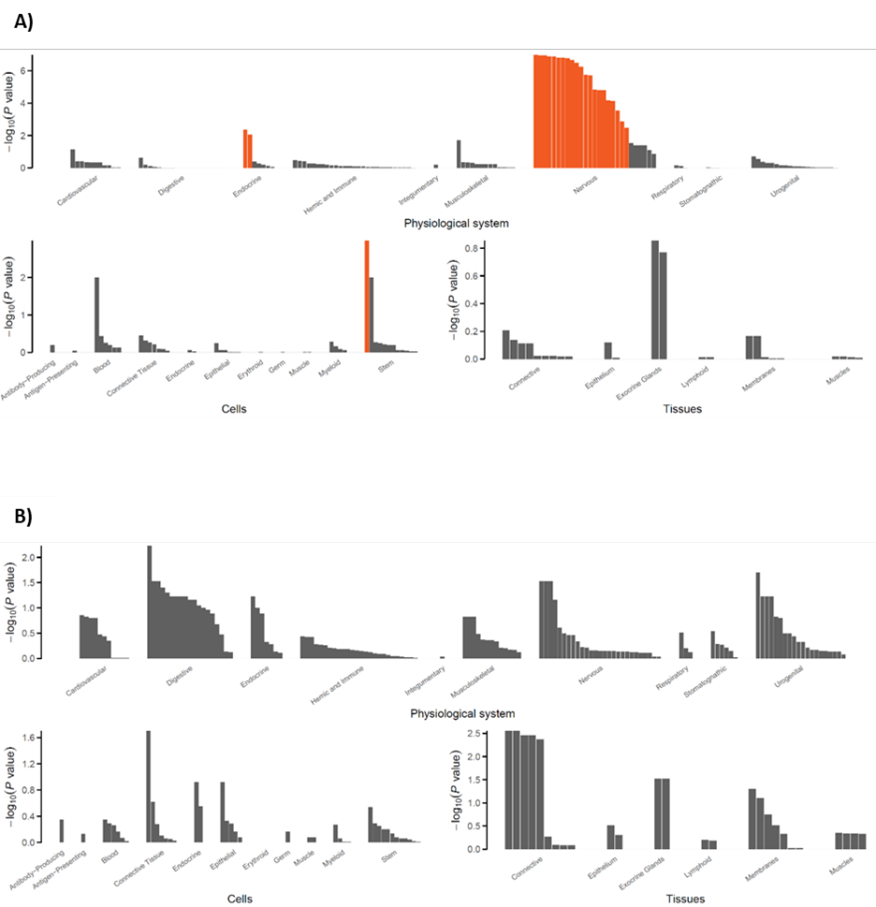
Figure legend: DEPICT cell, tissue and system enrichment bar plots for BMI-sedentary time analysis.
Having established that the two groups of genetic variants likely represent tissue-specific groups, we re-estimated the causal relationship between BMI and sedentary time using CAUSE, separately for the two groups of variants. We found that the 12,266 “brain-specific” genetic variants showed a significant causal effect on sedentary time (P=0.003), but the effect was attenuated compared to the CAUSE analysis where all 12,790 variants (i.e. also including the 524 “adipose tissue-specific” variants) were included in the analysis (P=6.3.x10-4). The statistical power was much more limited for the “adipose tissue-specific” variants, and we did not find a statistically significant causal relationship between BMI and sedentary time using the 524 “adipose tissue-specific” variants only (P=0.19). However, the direction of the effect suggested the possibility of a causal effect in case a stronger genetic instrument was available. Taken together, our analyses suggest that both brain-enriched and adipose tissue-enriched genetic variants are likely to show a causal relationship between BMI and sedentary time, which would suggest that the causal relationship between BMI and sedentary time is unlikely to be driven by an unobserved heritable factor.
Minor comments
The term "causally associated" are confusing, e.g. in l32. If it's causal, then use the term "causal".
We have now changed the term “causally associated” to “causal” throughout the manuscript.
Reviewer #3 (Public Review):
Given previous reports of an observational relationship between physical inactivity and obesity, Carrasquilla and colleagues aimed to investigate the causal relationship between these traits and establish the direction of effect using Mendelian Randomization. In doing so, the authors report strong evidence of a bidirectional causal relationship between sedentary time and BMI, where genetic liability for longer sedentary time increases BMI, and genetic liability for higher BMI causally increases sedentary time. The authors also give evidence of higher moderate and vigorous physical activity causally reducing BMI. However they do note that in the reverse direction there was evidence of horizontal pleiotropy where higher BMI causally influences lower levels of physical activity through alternative pathways.
The authors have used a number of methods to investigate and address potential limiting factors of the study. A major strength of the study is the use of the CAUSE method. This allowed the authors to investigate all exposures of interest, in spite of a low number of suitable genetic instruments (associated SNPs with P-value < 5E-08) being available, which may not have been possible with the use of the more conventional MR methods alone. The authors were also able to overcome sample overlap with this method, and hence obtain strong causal estimates for the study. The authors have compared causal estimates obtained from other MR methods including IVW, MR Egger, the weighted median and weighted mode methods. In doing so, they were able to demonstrate consistent directions of effects for most causal estimates when comparing with those obtained from the CAUSE method. This helps to increase confidence in the results obtained and supports the conclusions made. This study is limited in the fact that the findings are not generalizable across different age-groups or populations - although the authors do state that similar results have been found in childhood studies. As the authors also make reference to, due to the nature of the BMI genetic instruments used, the findings of this study can only inform on the lifetime impact of higher BMI, and not the effect of a short-term intervention.
The findings of this study will be of interest to those in the field of public health, and support current guidelines for the management of obesity.
We thank the Reviewer for the valuable feedback and insights. We agree that the lack of generalizability of the findings across age groups and populations is an important limitation. We have now mentioned this in lines 341-342 of the manuscript:
“The present study is also limited in the fact that the findings are not generalizable across different age-groups or populations.”
-
Evaluation Summary:
The manuscript by Carrasquilla and colleagues applied Mendelian Randomization (MR) techniques to study causal relationship of physical activity and obesity. Their results support the causal effects of physical activity on obesity, and bi-directional causal effects of sedentary time and obesity. One strength of this work is the use of CAUSE, a recently developed MR method that is robust to common violations of MR assumptions. The conclusion reached could potentially have a large impact on an important public health problem.
(This preprint has been reviewed by eLife. We include the public reviews from the reviewers here; the authors also receive private feedback with suggested changes to the manuscript. Reviewer #2 and Reviewer #3 agreed to share their name with the authors.)
-
Reviewer #1 (Public Review):
The authors employed a causal inference method known as Mendelian randomization (MR) to evaluate potential causal relationships between physical activities and obesity.
The main strength is that MR can provide evidence for causal relationships as it is less susceptible to reverse causality and confounding. The authors also employed a recently developed technique (CAUSE) that can leverage a very large number of genetic variants with increase in power.
There are no major flaws in the methodology as far as I observe. One limitation is that MR provides an effect size based on lifelong (from birth) exposure of the risk factor and may not reflect effects of increased physical exercise for a limited period of time (eg 3 months or 1 year). The findings are useful but may not be very novel or surprising given that …
Reviewer #1 (Public Review):
The authors employed a causal inference method known as Mendelian randomization (MR) to evaluate potential causal relationships between physical activities and obesity.
The main strength is that MR can provide evidence for causal relationships as it is less susceptible to reverse causality and confounding. The authors also employed a recently developed technique (CAUSE) that can leverage a very large number of genetic variants with increase in power.
There are no major flaws in the methodology as far as I observe. One limitation is that MR provides an effect size based on lifelong (from birth) exposure of the risk factor and may not reflect effects of increased physical exercise for a limited period of time (eg 3 months or 1 year). The findings are useful but may not be very novel or surprising given that many previous epidemiological studies also reach the same conclusion (that physical exercise help to reduce weight). Nevertheless, overall speaking, the methodology is sound and the results are supported by the analysis.
This work is clinically relevant as it provides further proof that physical exercise is causally related to lower BMI, while previous studies are not explicitly designed for causal inference. The study also provides estimates of (causal) effect sizes although the estimates may be larger than those from short-term interventions, as MR estimates reflect longer-term exposure.
-
Reviewer #2 (Public Review):
The manuscript by Carrasquilla and colleagues applied Mendelian Randomization (MR) techniques to study causal relationship of physical activity and obesity. Their results support the causal effects of physical activity on obesity, and bi-directional causal effects of sedentary time and obesity. One strength of this work is the use of CAUSE, a recently developed MR method that is robust to common violations of MR assumptions. The conclusion reached could potentially have a large impact on an important public health problem.
Major comments:
(1) While the effect of physical activity on obesity is in line with earlier studies, the finding that BMI has a causal effect on sedendary time is somewhat unexpected. In particular, the authors found this effect only with CAUSE, but the evidence from other MR methods do …
Reviewer #2 (Public Review):
The manuscript by Carrasquilla and colleagues applied Mendelian Randomization (MR) techniques to study causal relationship of physical activity and obesity. Their results support the causal effects of physical activity on obesity, and bi-directional causal effects of sedentary time and obesity. One strength of this work is the use of CAUSE, a recently developed MR method that is robust to common violations of MR assumptions. The conclusion reached could potentially have a large impact on an important public health problem.
Major comments:
(1) While the effect of physical activity on obesity is in line with earlier studies, the finding that BMI has a causal effect on sedendary time is somewhat unexpected. In particular, the authors found this effect only with CAUSE, but the evidence from other MR methods do not reach statistical significance cutoff. The strength of CAUSE is more about the control of false positive, instead of high power. In general, the power of CAUSE is lower than the simple IVW method. This is also the case in this setting, of high power of exposure (BMI) but lower power of outcome (sedentary time) - see Fig. 2B of the CAUSE paper.
It does not necessarily mean that the results are wrong. It's possible for example, by better modeling pleiotropic effects, CAUSE better captures the causal effects and have higher power. Nevertheless, it would be helpful to better understand why CAUSE gives high statistical significance while others not. Two suggestions here:
(a) It is useful to visualize the MR analysis with scatter plot of the effect sizes of variants on the exposure (BMI) and outcome (sedentary time). In the plot, the variants can be colored by their contribution to the CAUSE statistics, see Fig. 4 of the CAUSE paper. This plot would help show, for example, whether there are outlier variants; or whether the results are largely driven by just a small number of variants.
(b) CAUSE is susceptible to false positives when the value of q, a measure of the proportion of shared variants, is high. The authors stated that q is about 0.2, which is pretty small. However, it is unclear if this is q under the causal model or the sharing model. If q is small under the sharing model, the result would be quite convincing. This needs to be clarified.
(2) Given the concern above, it may be helpful to strengthen the results using additional strategy. Note that the biggest worry with BMI-sedantary time relation is that the two traits are both affected by an unobserved heritable factor. This hidden factor likely affects some behavior component, so most likely act through the brain. On the other hand, BMI may involve multiple tissue types, e.g. adipose. So the idea is: suppose we can partition BMI variants into different tissues, those acted via brain or via adipose, say; then we can test MR using only BMI variants in a certain tissue. If there is a causal effect of BMI on sedentary time, we expect to see similar results from MR with different tissues. If the two are affected by the hidden factor, then the MR analysis using BMI variants acted in adipose would not show significant results.
While I think this strategy is feasible conceptually, I realize that it may be difficult to implement. BMI heritability were found to be primarily enriched in brain regulatory elements [PMID:29632380], so even if there are other tissue components, their contribution may be small. One paper does report that BMI is enriched in CD19 cells [PMID: 28892062], though. A second challenge is to figure out the tissue of origin of GWAS variants. This probably require fine-mapping analysis to pinpoint causal variants, and overlap with tissue-specific enhancer maps, not a small task. So I'd strongly encourage the authors to pursue some analysis along this line, but it would be understandable if the results of this anlysis are negative.
Minor comments
- The term "causally associated" are confusing, e.g. in l32. If it's causal, then use the term "causal".
-
Reviewer #3 (Public Review):
Given previous reports of an observational relationship between physical inactivity and obesity, Carrasquilla and colleagues aimed to investigate the causal relationship between these traits and establish the direction of effect using Mendelian Randomization. In doing so, the authors report strong evidence of a bidirectional causal relationship between sedentary time and BMI, where genetic liability for longer sedentary time increases BMI, and genetic liability for higher BMI causally increases sedentary time. The authors also give evidence of higher moderate and vigorous physical activity causally reducing BMI. However they do note that in the reverse direction there was evidence of horizontal pleiotropy where higher BMI causally influences lower levels of physical activity through alternative pathways.
The …
Reviewer #3 (Public Review):
Given previous reports of an observational relationship between physical inactivity and obesity, Carrasquilla and colleagues aimed to investigate the causal relationship between these traits and establish the direction of effect using Mendelian Randomization. In doing so, the authors report strong evidence of a bidirectional causal relationship between sedentary time and BMI, where genetic liability for longer sedentary time increases BMI, and genetic liability for higher BMI causally increases sedentary time. The authors also give evidence of higher moderate and vigorous physical activity causally reducing BMI. However they do note that in the reverse direction there was evidence of horizontal pleiotropy where higher BMI causally influences lower levels of physical activity through alternative pathways.
The authors have used a number of methods to investigate and address potential limiting factors of the study. A major strength of the study is the use of the CAUSE method. This allowed the authors to investigate all exposures of interest, in spite of a low number of suitable genetic instruments (associated SNPs with P-value < 5E-08) being available, which may not have been possible with the use of the more conventional MR methods alone. The authors were also able to overcome sample overlap with this method, and hence obtain strong causal estimates for the study. The authors have compared causal estimates obtained from other MR methods including IVW, MR Egger, the weighted median and weighted mode methods. In doing so, they were able to demonstrate consistent directions of effects for most causal estimates when comparing with those obtained from the CAUSE method. This helps to increase confidence in the results obtained and supports the conclusions made.
This study is limited in the fact that the findings are not generalizable across different age-groups or populations - although the authors do state that similar results have been found in childhood studies. As the authors also make reference to, due to the nature of the BMI genetic instruments used, the findings of this study can only inform on the lifetime impact of higher BMI, and not the effect of a short-term intervention.The findings of this study will be of interest to those in the field of public health, and support current guidelines for the management of obesity.
-
