Early life experience sets hard limits on motor learning as evidenced from artificial arm use
Curation statements for this article:-
Curated by eLife

Evaluation Summary:
This is a large study of the development of human sensorimotor control using unique populations who have undergone limb loss at different times in their lives.This paper will be of interest to scientists within the field of motor control and for those interested in the development and plasticity of the motor system. An important finding is that reaching performance with an artificial arm is better in people who lost their limb in adulthood and worse in those with congenital limb loss. While the mechanisms underlying this result are not yet clear, it suggests that the benefits of early developmental experience with an intact limb are superior to early experience with an artificial arm.
(This preprint has been reviewed by eLife. We include the public reviews from the reviewers here; the authors also receive private feedback with suggested changes to the manuscript. The reviewers remained anonymous to the authors.)
This article has been Reviewed by the following groups
Discuss this preprint
Start a discussion What are Sciety discussions?Listed in
- Evaluated articles (eLife)
Abstract
The study of artificial arms provides a unique opportunity to address long-standing questions on sensorimotor plasticity and development. Learning to use an artificial arm arguably depends on fundamental building blocks of body representation and would therefore be impacted by early life experience. We tested artificial arm motor-control in two adult populations with upper-limb deficiencies: a congenital group—individuals who were born with a partial arm, and an acquired group—who lost their arm following amputation in adulthood. Brain plasticity research teaches us that the earlier we train to acquire new skills (or use a new technology) the better we benefit from this practice as adults. Instead, we found that although the congenital group started using an artificial arm as toddlers, they produced increased error noise and directional errors when reaching to visual targets, relative to the acquired group who performed similarly to controls. However, the earlier an individual with a congenital limb difference was fitted with an artificial arm, the better their motor control was. Since we found no group differences when reaching without visual feedback, we suggest that the ability to perform efficient visual-based corrective movements is highly dependent on either biological or artificial arm experience at a very young age. Subsequently, opportunities for sensorimotor plasticity become more limited.
Article activity feed
-

-

Author Response:
Reviewer #1:
Maimon-Mor et al. examined the control of reaching movement of one-handers, who were born with a partial arm, and amputees, who lost their arm in adulthood. The authors hypothesized that since one-handers started using their artificial arm earlier in life then amputees, they are expected to exhibit better motor control, as measured by point-to-point reaching accuracy. Surprisingly, they found the opposite, that the reaching accuracy of one-handers is worse than that of amputees (and control with their non-dominant hand). This deficit in motor control was reflected in an increase in motor noise rather than consistent motor biases.
Strengths:
- I found the paper in general very well and clearly written.
- The authors provide detailed analyses to examine various possible factors underlying deficits in …
Author Response:
Reviewer #1:
Maimon-Mor et al. examined the control of reaching movement of one-handers, who were born with a partial arm, and amputees, who lost their arm in adulthood. The authors hypothesized that since one-handers started using their artificial arm earlier in life then amputees, they are expected to exhibit better motor control, as measured by point-to-point reaching accuracy. Surprisingly, they found the opposite, that the reaching accuracy of one-handers is worse than that of amputees (and control with their non-dominant hand). This deficit in motor control was reflected in an increase in motor noise rather than consistent motor biases.
Strengths:
- I found the paper in general very well and clearly written.
- The authors provide detailed analyses to examine various possible factors underlying deficits in reaching movements in one-handers and amputees, including age at which participants first used an artificial arm, current usage of the arm, performance in hand localization tasks, and statistical methods that control for potential confounding factors.
- The results that one handers, who start using the artificial arm at early age, show worse motor control than amputees, who typically start using the arm during adulthood, are surprising and interesting. Also intriguing are the results that reaching accuracy is negatively correlated with the time of limbless experience in both groups. These results suggest that there is a plasticity window that is not anchored to a certain age, but rather to some interference (perhaps) from the time without the use of artificial arm. In one-handers these two time intervals are confounded by one another, but the amputees allow to separate them. I think that the results have implications for understanding plasticity aspects of acquiring skills for using artificial limbs.
Weaknesses:
- While I found that one of the main conclusion from the paper is that the main factor that is related to increased motor noise is the time spent without the artificial arm, it felt that this was not emphasized as such. These results are not mentioned in the abstract and the correlation for amputees is not shown in a figure.
We thank the reviewer for their comment. While it is true that motor noise correlated with time of limbless experience in both groups, we were hesitant to highlight the results found in amputees, considering the small number of participants, and lack of converging evidence (e.g., contrary to the congenital group, we did not find a strong main effect). For these reasons, we have chosen to include it in the manuscript but not highlight it or base our main conclusions on it. Following the reviewer’s comment, the correlation of the amputees’ data is now visualised in Figure 3. Moreover, while the behavioural correlation might be similar in both groups, from a neural standpoint, the limbless experience of a toddler with a developing brain is qualitatively different to that of an adult, with a fully developed brain, who has lost a limb. As such, we were hesitant to link these two findings into a single framework, however in the revised manuscript we highlight this tentative link.
Discussion (4th paragraph):
“In both the congenital and acquired groups, artificial arm reaching motor noise correlated with the amount of time they spent using only their residual limb. It is therefore tempting to link these two results under a unifying interpretation; however, this requires further research, considering the neural differences between the two groups.”
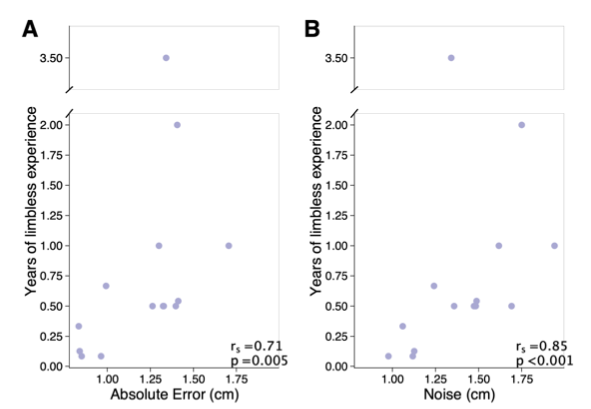
Figure 3. Years of limbless experience before first artificial arm use in the acquired group. (A) Relationship between years of limbless experience and (A) artificial arm reaching errors or (B) artificial arm motor noise in the acquired group.
- The suggested mechanism of a deficit in visuomotor integration is not clear, and whether the results indeed point to this hypothesis. The results of the reaching task show that the one-handers exhibit higher motor noise and initial error direction than amputees. The results of the 2D localization task (the same as the standard reaching task but without visual feedback) show no difference in errors between the groups. First, it is not clear how the findings of the 2D localization task are in line with the results that one-handers show larger initial directional errors.
We fully take on the reviewer’s comment regarding the vague use of the term visuomotor integration. In the revised manuscript, we have opted instead for a much broader term, suggesting a deficit in visual-based corrective movements, considering we are limited in our ability to infer the specific underlying mechanism from our result. We have also made changes to the abstract based on the reviewer’s comment (see below).
With regards to discussing how the various results fit together, in the revised manuscript, these are now discussed more at length. In short, in the 2D localisation task (reaching without visual feedback), participants were not instructed to perform fast ballistic movements. Instead, participants were instructed that they could perform movements to correct for their initial aiming error (using proprioception). Together with the similar performance observed for the proprioceptive task, this strengthens our suggestion that the deficit in the congenital group is triggered by visual-driven corrections. These various considerations are now detailed as follows:
Abstract:
“Since we found no group differences when reaching without visual feedback, we suggest that the ability to perform efficient visually-based corrective movements, is highly dependent on either biological or artificial arm experience at a very young age.”
Result (section 7, 1st paragraph):
“From these results, we infer that early-life experience relates to a suboptimal ability to reduce the system’s inherent noise, and that this is possibly not related to the noise generated by the execution of the initial motor plan. Early life experience might therefore relate to better use of visual feedback in performing corrective movements. The continuous integration of visual and sensory input is at the heart of visually- driven corrective movements. Therefore, one possibility is that limited early life experience, results in suboptimal integration of information within the sensorimotor system.”
Discussion (2nd paragraph):
“When performing reaching movements without visual feedback (2D localisation task), the congenital group did not differ from the acquired or control group. This begs the question, if the congenital group has a deficit in motor planning why was it not evident in this task as well? In the 2D localisation task, unlike the main task, participants were allowed to make corrective movements. While they did not receive visual feedback, the proprioceptive and somatosensory feedback from the residual limb appears to be enough to allow them to correct for initial reaching errors and perform at the same level as the acquired and control group. Moreover, we did not find strong evidence for an impaired sense of localisation of either the residual or the artificial arm in the congenital group. As such, by elimination, our evidence suggests that the process of using visual information to perform corrective movements isn’t as efficient in the congenital group.”
Discussion (2nd paragraph):
“Lack of concurrent visual and motor experience during development might therefore cause a deficit in the ability to form the computational substrates and thus to efficiently use visual information in performing corrective movements.”
Discussion (last paragraph):
“By the process of elimination, we have nominated suboptimal visual feedback-based corrections to be the most likely cause underlying this motor deficit.”
Second, I think that these results suggest that the deficiency in one-handers is with feedback responses rather than feedforward. This may also be supported by the correlation with age: early age is correlated with less end-point motor noise, rather than initial directional error. Analyses of feedback correction might help shedding more light on the mechanism. The authors mention that the participants were asked to avoid doing corrective movement and imposed a limit of 1 sec per reach to encourage that. But it is not clear whether participants actually followed these instructions. 1 sec could be enough time to allow feedback responses, especially for small amplitude movements (e.g., <10 cm).
Please see below our response to the feedback correction analysis suggestion. Regarding corrective movements, we had the same concern as the reviewer which led us to use hand velocity data to identify first movement termination. We apologise if the experimental design and pre-processing procedures were not clear.
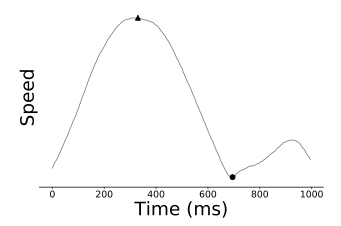
In short, a 1 sec trial duration was imposed on all trials to generate a sense of time- pressure and encourage participants to perform fast ballistic movements. As we were worried that participants might still perform secondary corrective movements within this 1 sec window, for each trial, we used the hand velocity profile to identify the end of the first movement. Below, we have plotted the arm velocity from a single trial to illustrate this procedure. For this trial, the timepoint indicated by the circular marker has been identified as the time of the end of the first movement (See Methods for further information). For each trial, endpoint location was defined as the location of the arm at the movement termination timepoint defined by the kinematic data and not the endpoint at the 1 sec timepoint. It is worth noting that performing the same analysis using the end- points recorded at the 1 sec timepoint did not generate different statistical results.
This has now been further clarified in the text.
Results (section 1, 1st paragraph):
“Reaching performance was evaluated by measuring the mean absolute error participants made across all targets (see Figure 1C). The absolute error refers to the distance from the cursor’s position at the end of the first reach (endpoint) to the centre of the target in each trial. The endpoint of each trial was set as the arm location at the end of the first reaching movement, identified using the trial’s kinematic data (See Methods).”
Methods (section: Data processing and analysis – main task):
“Within the 1 sec movement time constraint, in some trials, participants still performed secondary corrective movements. We therefore used the tangential arm velocities to identify the end of the first reach in each trial (i.e., movement termination).”
Reviewer #2:
This is a broad and ambitious study that is fairly unique in scope - the questions it seek to answer are difficult to answer scientifically, and yet the depth of the questions it seeks to answer and the framework in which it is founded seem out of place in a clinical journal.
And yet, as a scientist and clinician, I found myself objecting to the claims of the authors, only have them to address my objection in the very next section. The results are surprising, but compelling - the authors have done an excellent job of untangling a very complicated question, and they have tested (for our field) a large number of subjects.
The main two results of the paper, from my perspective, are as follows:
- Persons with an amputation can form better models of new environments, such as manipulandums, than can those with congenital deficiencies. This result is interesting because a) the task did not depend on significant use of the device (they were able to use their intact musculature for the reaching-based task), and b) the results were not influenced by the devices used by the subjects (cosmetic, body-powered, or myoelectric).
- Persons with congenital deficiency fit earlier in life had less error than those fit later in life.
Taken together, these results suggest that during early childhood the brain is better able to develop the foundation necessary to develop internal models and that if this is deprived early in childhood, it cannot be regained later in life - even if subjects have MORE experience. (E.g., those with congenital deficiencies had more experience using their prosthetic arm than those with amputation, and yet scored worse).
The questions analyzed by the researchers are excellent and the statistical methods are generally appropriate. My only minor concern is that the authors occasionally infer that two groups are the same when a large p-value is reported, whereas large p-values do not convey that the groups are the same; only that they cannot be proven to be different. The authors would need to use a technique such as ICC or analysis of similarities to prove the groups are the same.
We appreciate the reviewer’s concern about inferring the null from classical frequentist statistics. In this manuscript, we have opted to using Bayesian statistics as a measure of testing the significance of similarity across groups (See Methods: Statistical analysis) as opposed to the frequentist methods suggested by the reviewer. This approach is equivalent to the ones proposed by the reviewer and are widely used in our field. A Bayesian Factor (BF) smaller than 0.33 is regarded as sufficient evidence for supporting the null hypothesis that is, that there are no differences between the groups.
This approach is described in detail in the methods and is introduced in the first section of the results as well.
Results (1st section 2nd paragraph):
“To further explore the non-significant performance difference between amputees and controls, we used a Bayesian approach (Rouder et al., 2009), that allows for testing of similarities between groups (the null hypothesis). In this analysis, the smaller effect size of the two reported here (1.39) was inputted as the Cauchy prior width. The resulting Bayesian Factor (BF10=0.28) provided moderate support to the null hypothesis (i.e., smaller than 0.33).”
Methods (Statistical analysis section):
“In parametric analyses (ANCOVA, ANOVA, Pearson correlations), where the frequentist approach yielded a non-significant p-value, a parallel Bayesian approach was used and Bayes Factors (BF) were reported (Morey & Rouder, 2015; Rouder et al., 2009, 2012, 2016). A BF<0.33 is interpreted as support for the null-hypothesis, BF > 3 is interpreted as support for the alternative hypothesis (Dienes, 2014). In
Bayesian ANOVAs and ANCOVA’s, the inclusion Bayes Factor of an effect (BFIncl) is reported, reflecting that the data is X (BF) times more likely under the models that include the effect than under the models without this predictor. When using a Bayesian t-test, a Cauchy prior width of 1.39 was used, this was based on the effect size of the main task, when comparing artificial arm reaches of amputees and one- handers. Therefore, the null hypothesis in these cases would be there is no effect as large as the effect observed in the main task.”
Following the reviewer’s comment, we have carefully scanned through the manuscript to make sure no equivalence claims are made without the support of a significant BF. In one instance that has been the case and has been rectified.
Results (3rd section, 2nd paragraph):
“We compared artificial arm and nondominant arm biases (distance from the centre of the endpoint to the target) across groups, using intact arm biases as a covariate. The ANCOVA resulted in no significant (inconclusive) group differences (F(2,47)=2.40, p=0.1, BFIncl=0.72; see Figure 2A).”
-
Reviewer #2 (Public Review):
This is a broad and ambitious study that is fairly unique in scope - the questions it seek to answer are difficult to answer scientifically, and yet the depth of the questions it seeks to answer and the framework in which it is founded seem out of place in a clinical journal.
And yet, as a scientist and clinician, I found myself objecting to the claims of the authors, only have them to address my objection in the very next section. The results are surprising, but compelling - the authors have done an excellent job of untangling a very complicated question, and they have tested (for our field) a large number of subjects.
The main two results of the paper, from my perspective, are as follows:
Persons with an amputation can form better models of new environments, such as manipulandums, than can those with …
Reviewer #2 (Public Review):
This is a broad and ambitious study that is fairly unique in scope - the questions it seek to answer are difficult to answer scientifically, and yet the depth of the questions it seeks to answer and the framework in which it is founded seem out of place in a clinical journal.
And yet, as a scientist and clinician, I found myself objecting to the claims of the authors, only have them to address my objection in the very next section. The results are surprising, but compelling - the authors have done an excellent job of untangling a very complicated question, and they have tested (for our field) a large number of subjects.
The main two results of the paper, from my perspective, are as follows:
Persons with an amputation can form better models of new environments, such as manipulandums, than can those with congenital deficiencies. This result is interesting because a) the task did not depend on significant use of the device (they were able to use their intact musculature for the reaching-based task), and b) the results were not influenced by the devices used by the subjects (cosmetic, body-powered, or myoelectric).
Persons with congenital deficiency fit earlier in life had less error than those fit later in life.
Taken together, these results suggest that during early childhood the brain is better able to develop the foundation necessary to develop internal models and that if this is deprived early in childhood, it cannot be regained later in life - even if subjects have MORE experience. (E.g., those with congenital deficiencies had more experience using their prosthetic arm than those with amputation, and yet scored worse).
The questions analyzed by the researchers are excellent and the statistical methods are generally appropriate. My only minor concern is that the authors occasionally infer that two groups are the same when a large p-value is reported, whereas large p-values do not convey that the groups are the same; only that they cannot be proven to be different. The authors would need to use a technique such as ICC or analysis of similarities to prove the groups are the same.
-
Reviewer #1 (Public Review):
Maimon-Mor et al. examined the control of reaching movement of one-handers, who were born with a partial arm, and amputees, who lost their arm in adulthood. The authors hypothesized that since one-handers started using their artificial arm earlier in life then amputees, they are expected to exhibit better motor control, as measured by point-to-point reaching accuracy. Surprisingly, they found the opposite, that the reaching accuracy of one-handers is worse than that of amputees (and control with their non-dominant hand). This deficit in motor control was reflected in an increase in motor noise rather than consistent motor biases.
Strengths:
I found the paper in general very well and clearly written.
The authors provide detailed analyses to examine various possible factors underlying deficits in reaching …
Reviewer #1 (Public Review):
Maimon-Mor et al. examined the control of reaching movement of one-handers, who were born with a partial arm, and amputees, who lost their arm in adulthood. The authors hypothesized that since one-handers started using their artificial arm earlier in life then amputees, they are expected to exhibit better motor control, as measured by point-to-point reaching accuracy. Surprisingly, they found the opposite, that the reaching accuracy of one-handers is worse than that of amputees (and control with their non-dominant hand). This deficit in motor control was reflected in an increase in motor noise rather than consistent motor biases.
Strengths:
I found the paper in general very well and clearly written.
The authors provide detailed analyses to examine various possible factors underlying deficits in reaching movements in one-handers and amputees, including age at which participants first used an artificial arm, current usage of the arm, performance in hand localization tasks, and statistical methods that control for potential confounding factors.
The results that one handers, who start using the artificial arm at early age, show worse motor control than amputees, who typically start using the arm during adulthood, are surprising and interesting. Also intriguing are the results that reaching accuracy is negatively correlated with the time of limbless experience in both groups. These results suggest that there is a plasticity window that is not anchored to a certain age, but rather to some interference (perhaps) from the time without the use of artificial arm. In one-handers these two time intervals are confounded by one another, but the amputees allow to separate them. I think that the results have implications for understanding plasticity aspects of acquiring skills for using artificial limbs.
Weaknesses:
While I found that one of the main conclusion from the paper is that the main factor that is related to increased motor noise is the time spent without the artificial arm, it felt that this was not emphasized as such. These results are not mentioned in the abstract and the correlation for amputees is not shown in a figure.
The suggested mechanism of a deficit in visuomotor integration is not clear, and whether the results indeed point to this hypothesis. The results of the reaching task show that the one-handers exhibit higher motor noise and initial error direction than amputees. The results of the 2D localization task (the same as the standard reaching task but without visual feedback) show no difference in errors between the groups. First, it is not clear how the findings of the 2D localization task are in line with the results that one-handers show larger initial directional errors. Second, I think that these results suggest that the deficiency in one-handers is with feedback responses rather than feedforward. This may also be supported by the correlation with age: early age is correlated with less end-point motor noise, rather than initial directional error. Analyses of feedback correction might help shedding more light on the mechanism. The authors mention that the participants were asked to avoid doing corrective movement and imposed a limit of 1 sec per reach to encourage that. But it is not clear whether participants actually followed these instructions. 1 sec could be enough time to allow feedback responses, especially for small amplitude movements (e.g., <10 cm).
-
Evaluation Summary:
This is a large study of the development of human sensorimotor control using unique populations who have undergone limb loss at different times in their lives.This paper will be of interest to scientists within the field of motor control and for those interested in the development and plasticity of the motor system. An important finding is that reaching performance with an artificial arm is better in people who lost their limb in adulthood and worse in those with congenital limb loss. While the mechanisms underlying this result are not yet clear, it suggests that the benefits of early developmental experience with an intact limb are superior to early experience with an artificial arm.
(This preprint has been reviewed by eLife. We include the public reviews from the reviewers here; the authors also receive private …
Evaluation Summary:
This is a large study of the development of human sensorimotor control using unique populations who have undergone limb loss at different times in their lives.This paper will be of interest to scientists within the field of motor control and for those interested in the development and plasticity of the motor system. An important finding is that reaching performance with an artificial arm is better in people who lost their limb in adulthood and worse in those with congenital limb loss. While the mechanisms underlying this result are not yet clear, it suggests that the benefits of early developmental experience with an intact limb are superior to early experience with an artificial arm.
(This preprint has been reviewed by eLife. We include the public reviews from the reviewers here; the authors also receive private feedback with suggested changes to the manuscript. The reviewers remained anonymous to the authors.)
-
